
The odds of developing clinical depression over one’s lifetime are, roughly, 30%. The odds of a relapse, once you have experienced depression, is about 50%. And, at any one time, perhaps around 5% of people suffer from depression. So, depression is common and prevalent.
All that is to say that if you happen to be a Pilot or an Air Traffic Controller and have the misfortune to get depressed at some point in your career…you are fairly screwed. Now, before I describe why, for simplicity’s sake let’s just talk about pilots; essentially everything I am about to say would apply equally to an Air Traffic Controller. And simplicity, in this case, is a blessing; the FAA regulations are so complex that they will make your head spin.
Here are the basics. Commercial and airline pilots need to get medically recertified every 6 to 12 months, depending on their age. Private pilots need to get the clearance every 2 to 5 years. The process entails filling out a form – the 8500-8 – and paying to meet with an Aviation Medical Examiner (AME).
An AME screens the pilot for any new or preexisting health condition that might interfere with the pilot’s judgment or abilities. There are a lot of issues that could draw the physician’s attention: a new cardiac event, a stroke, kidney stones, etc. If the AME doctor learns of a disorder, the pilot’s renewal is either outright rejected or, much more commonly, deferred. This is all very reasonable – we do not want pilots flying planes when they lose their depth perception or some such thing. All-in-all, around 6% of pilots get identified as having a health condition requiring a FAA-exemption. For nearly all, the finding results in a significant delay in licensure but, rarely, a denial.
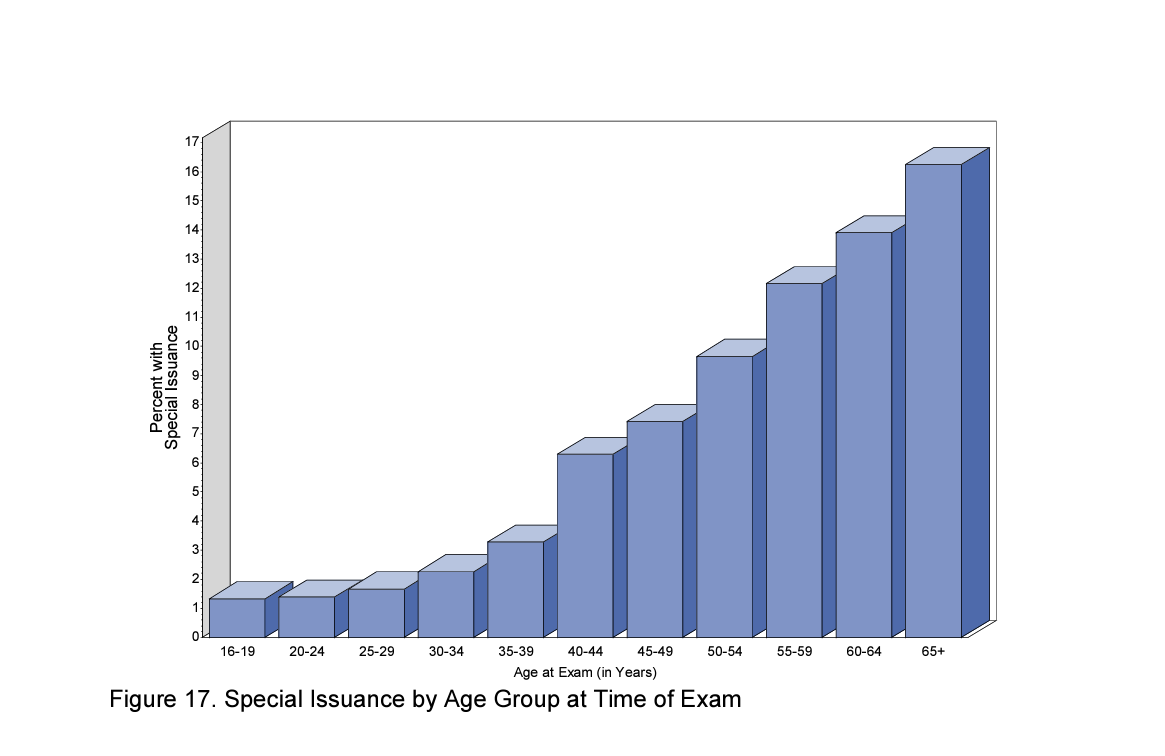
And, as a side-note, it is worth observing that, in this case, age is not a pilot’s friend. As pilots get older, they may become wiser and more experienced. But, they are also more likely to run afoul of the FAA policy and need a medical exemption.
(DOT/FAA/AM-23-38 2022 Aerospace Medical Certification Statistical Handbook)
What, then, are the common reasons pilots get referred to the FAA for a special license? What are the most common medical conditions? Substance use, hypertension, and allergies. Of around the 590,000 licensed pilots in 2022, about 38,000 were flagged for substance use.
At this point, it bears noting that the AME is not the pilot’s doctor. Although the pilot arranges for and pays for the exam, the AME actually works for the federal government – the FAA. The exam is shared with the FAA and, when an issue is discovered, the AME does not treat the pilot; they report the pilot’s health issue up the chain to Washington, D.C.
In psychiatry, this is the equivalent of a forensic evaluation. It is an exam done for someone else to certify or provide expert testimony. Forensic exams may be friendly but, at root, they are adversarial. When seeing the doctor people will, with good reason, neglect details, avoid embarrassing or damaging admissions…all that. It is to be expected. That is why forensic exams usually include some reality checks – testing for confabulation or lying, verification and reviews of documentation, labs, and medical records. All sorts of secondary data.
So, with that background, let’s briefly discuss alcohol and drug use. Patients will often minimize their use of substances. Way back in my residency, I was taught some bit of clinical lore: When considering if alcohol use might be a problem, ask how much alcohol is consumed each week. Then, double it. Even if the drinking does not matter to one’s job security, marriage, or really anything external, it still matters to one’s self-image. Generally, people will minimize it.
But, when the amount consumed actually does matter – when your job depends on the answer you give – people will almost always minimize the alcohol use, if they can.
So, back to pilots. In a recent dataset, around 1,500 pilots were being monitored for substance use. Around 28% were self-referred. The other 72% were identified by other means – chiefly drunk driving (24%). Around 93% were there for alcohol; the remaining 7% for other substances. ( C Ohmsieder, Q Snyder, B Petersen, 9/16/24, HIMS Overview, 2024 Basic Education Seminar. Denver CO.)
With these pilots, the FAA identified a bunch of substance issues through the AME. About a fourth of them seemed to be help-seeking as they admitted to the issue; the rest were “discovered” through the process. Pretty much all then get their licenses deferred. What then? Treatment.
We have well-established methods to treat substance abuse. We also have medications that can help in the process, though pilots may not be allowed to use many of them. So what may be surprising is that the FAA’s approach to the treatment and rehabilitation of its pilots is a success story. Why? Because with alcohol, the FAA can monitor and detect its use. Labs can measure alcohol use for hours (Ethanol), days/weeks (EtG/EtS, CDT, PEth) and months (FAEE) after consumption. And those docs caring for someone in, say, an alcohol rehabilitation clinic, perform these tests: “Trust but verify.”
As there are clear markers of ongoing use that can be tested – and the pilots who have been identified as having substance use issues are tested at least 14 times every year– the recovery and abstinence rate among pilots is remarkable. The FAA measures a relapse rate with alcohol at around 13% – far lower than the roughly 60% relapse seen in the general public.
And, remember, this is a cohort that, for three-quarters of them, did not seek out help for their problem; they were discovered or reported on. Generally, people forced into treatment do worse.
So, these numbers are relatively stunning. I don’t know. Maybe the data is distorted by not accounting for those who just gave up on piloting and never tried to get sober? Regardless, the forensic role of the AME, the FAA’s firm policy, the implementation of a well-established program, and the ability to test for relapse works really, really well.
But, as we shall see, if the FAA demonstrates a good balance between treatment and enforcement with substance use, it falls flat when it comes to managing depression within the cockpit.
Unlike a broken bone, an abnormal x-ray, or a “hot” UA, there are no dependable tests for depression. It is a feeling, not a lab result and, absent some external manifestation like a suicide attempt or some self-harm behavior, the diagnosis generally requires self-reporting.
Of course, there are exceptions. Yes, if one has a severe “melancholic depression,” most clinicians will pick it up. It is hard to hide. But, an “atypical depression” – perversely named as it is probably the most typical form of depression – can be much less evident. And, in a profession where you are not permitted to work if you are depressed, you survive by hiding your emotions. That is the culture and reality of piloting.
So, while enforcement and testing works with other demonstrable and measurable medical illnesses, it fails with depression. As per the FAA, in 2022 around three in every thousand pilots were being treated by antidepressants. How does this compare to the general US public? Roughly one in every nine people use an antidepressant. That would make pilots 40-times less likely to have a medication prescribed for their mood then others in our society. You can nitpick the numbers and challenge the data but the multiples are massive. Adjusting for this or that still leads you to the same conclusion: there is a deep pool of untreated depression among pilots.
It is fair to say and widely acknowledged that depression in pilots is underreported, undertreated, and/or deeply buried underground. There are loads of pilots that are depressed but never get treatment. There are also pilots that get treatment but never report it to the FAA – risking a federal crime. Looping back to substance use – there are a whole lot of pilots that self-medicate their depression with alcohol.
Soon, we will dive deeper into how the FAA (mis)manages depression, when it is detected. But, first, in Part 2, we will discuss German Wings Flight 9525 and other sentinel events and how they inform and complicate the FAA’s task.